
A pneumothorax is the medical word for the condition when air leaks through a defect in the lung, the chest wall or both, and collects in the pleural space. There are several types of pneumothorax but all patients will have respiratory problems and be in pain. Traumatic pneumothoraxes are divided into open and closed types. An open pneumothorax occurs when there is open communication between the environment and the pleural cavity through the chest wall. A special type of open pneumothorax — and the one we’re discussing here — is a sucking chest wound. In the sucking chest wound, air is sucked into the thoracic cavity through the chest wall instead of into the lungs through the airways. This is the type of injury you get if you’re impaled or shot.
The old school treatment (do you remember from your FirstAid class?) had us taping a piece of plastic or Saran wrap over the site/hole, injury. It was called an air-occlusive dressing and we were shown how to tape it on three sides. It was thought that this dressing prevented additional air from entering the pleural cavity during inhalation and allowed trapped air to escape from the untaped edge during exhalation. However, according to JEMS, the time required to apply this dressing and the limited effectiveness of the adhesive to stick to a bleeding, often hairy, patient regularly resulted in dressing failure.
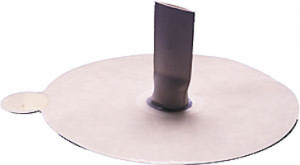
Because of these difficulties, the Asherman Chest Seal was developed. This single-step dressing includes a tube with a one-way valve that extends from the center to allow air to escape—similar to the three-sided dressing but with a reduction in the amount of time needed for application.
The Asherman Chest Seal (ACS) is available online for about $15. It is standard issue for the US Army, US Navy and the British Army for use in emergency situations with open pneumothorax wounds (sucking chest wounds). The ACS is the one item every responder needs for the field treatment of open chest wounds. It features a circular design and one-way valve designed to let air and blood escape while preventing either from reentering. The clear pad design allows for a provider to easily monitor the wound. The strong pressure sensitive adhesive will create an effective seal regardless of amount of body hair.
An alternative emergency approach to this dressing is to simply place an AED defibrillator pad on the wound, should one be available. Although it doesn’t allow for escape of pleural air, the pad’s adhesive resolves the problems of too much time needed to tape three sides of the dressing and failure of the adhesive to stick to the patient’s bloody chest wall. In some settings, this simple approach combined with occasional “burping” of the dressing, is the best way to go.